Multiple breathing tests. A mask covering the face. Continuous consumptions of medications.
That’s the life of a cystic fibrosis patient.

I’ve never really understood the term “limited life” until I learned about cystic fibrosis. Several precautions need to be made, you’re not allowed to do things that may affect your health, and you always need to be on top of the game for health. This disease is very rare but known worldwide. I asked a couple of people about this disease, and the answer was either: a) I’ve only heard about the disease b) Yeah, somewhat. (But in reality, all they knew was that it’s something about the lungs)
But I also noticed that very few responded with “I have cystic fibrosis”. A person can be diagnosed with CF as early as the age of 2 months, and usually have a lifespan of 38 years. In my opinion, that isn’t the longest life, and within those years, they’ll probably be spending most of their time with a nebulizer (a machine used to improve tension and muscular activity within lung airways or chest).
Cystic Fibrosis isn’t just the easiest disease to treat. For every patient, there’s a different problem, a different outcome, and a different situation. The best way to approach a disease is to have the best treatment and to have the best treatment, it needs to be personalized.
Cystic fibrosis is a rare genetic disease, that affects different organs — lungs, liver, pancreas, etc. CF causes mutations within cells that produce mucus, leading to severe problems within the organs.

Most patients are diagnosed with CF in the lungs. Due to its complex structure and fragility, the disease is quite difficult to diagnose. The basic formation of the lungs can look like 2 sponges connected together with a bunch of pipes. That’s just a basic level of the lung structure that even a pre-schooler can understand. The lungs are in constant movement because of their continuous supply of oxygen.
The journey of oxygen starts with a somewhat long pipe, running down in your neck, known as the trachea, located in the neck. As the trachea runs down near the lungs, it divides into 2 separate pipes, known as the bronchi. And finally, seeping into the sponge lung materials, the smaller branches called bronchioles are wrapped around tiny sacs, alveoli.
Oxygen inhaled in the body is brought into the alveoli, where capillaries are surrounding the tiny sacs. When a person breathes, exchanges between the alveoli (oxygen-stored) and the capillaries (takes out carbon dioxide) occurs.
While oxygen runs through the airways, it passes through a slimy substance, known as mucus, which is coated along the perimeter. Mucus plays a huge role in the lungs, by acting as a janitor. It captures most of the germs, and dust that were mixed in with oxygen, and is taken out and replaced with the new layer each time.
- When air is inhaled, it’s cleaned by a layer of mucus in the airways
People with CF, have a much different experience, where mucus comes in uninvited. For a CF patient, mucus is thicker than normal, thereby cilia are unable to move the substance out of the airway. That’s like asking an ant to push over an elephant (Nearly impossible). Now, we’re left with heavy sticky mucus, just covering the airways, and as this mucus builds up, it can result in clogs, or even produce bacteria since pollutants are stored. Inside of cleaning the air, mucus damages the airways, and oxygen can’t efficiently reach parts of the body, such as the alveoli.
CFTR Protein
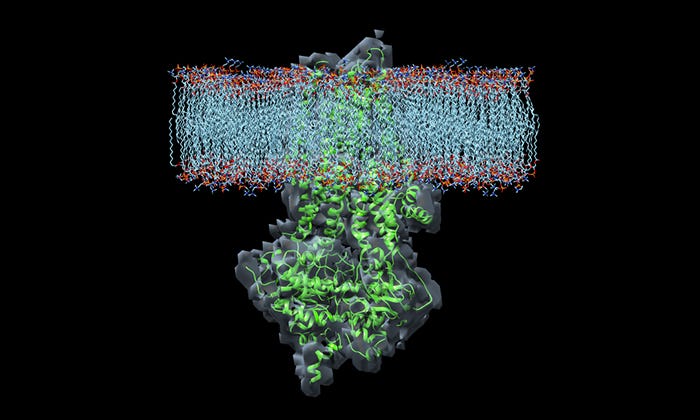
CFTR Protein, aka Cystic fibrosis transmembrane conductance regulator protein, is a special type of protein that assists in balancing 3 materials, chloride, sodium, and water. Similar to all proteins, CFTR proteins are formed through 3 main stages: Transcription, translation, trafficking.
DNA in the cell consists of instructions to form the protein, and mRNA starts to replicate this protein (transcription). As the RNA collides with the ribosome, it begins to match the coded instructions, in a process called translation. Ribosomes, mRNA, and tRNA are brought together where strands of amino acids are linked, and form a protein, in this case, CFTR Proteins. Next, the CFTR protein locates itself to the cell membrane, and this is known as trafficking. CFTR Proteins act like border officers and allow specific molecules to pass through the cell’s borderlines. and becomes a channel to transport molecules between the cell’s borderlines.
In the scenario of cystic fibrosis, things seem to get out of “hand”. Just like having a puzzle with missing pieces is known to be an incomplete picture, the same concept goes with the genetics of CF.
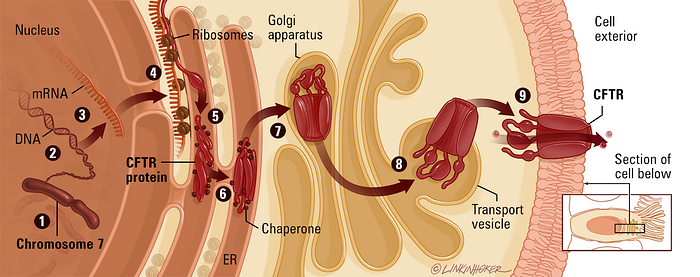
The CFTR gene has 27 exons, and one of these exons determine the structure of a CFTR Protein:
- The DNA strand that codes the protein is replicated by RNA. Components that are not needed, are taken out, resulting in an mRNA
- The mRNA travels to the endoplasmic reticulum (ER) and binds with ribosomes to be translated into a protein
- Travels to the Golgi apparatus (GA). Proteins, known as chaperones, help shape the protein and add sugars.
- Locates to the surface of the cell, and channels ions within the cell membrane
Thousands of mutations have been recognized, and one of the most common mutations in the CFTR protein is called F508DEL. This mutation occurs when 3 nucleotides are deleted from the DNA (positions 507 and 508). These 3 genes are responsible for creating phenylalanine, which is an important amino acid, that contributes to the CFTR protein. Though the protein is made of over 1,480 amino acids, the protein can behave abnormally due to the lack of specific amino acids, called phenylalanine. Without phenylalanine, CFTR protein isn’t structured properly and may form an abnormal 3D shape. In some cases, the Golgi apparatus identifies this and analyzes the protein structure irregular shape, which leads to the protein degraded in the organelle. In CF, the protein is either killed, damaged, or is faulty.
→ Cystic Fibrosis: dysfunctional CFTR Protein
A normal CFTR protein usually has 5 main components:
- 2 transmembrane domains — TMD1 + TMD2
- 2 cytoplasmic nucleotide-binding domains — NBD1 + NBD2
- 1 regulatory domain
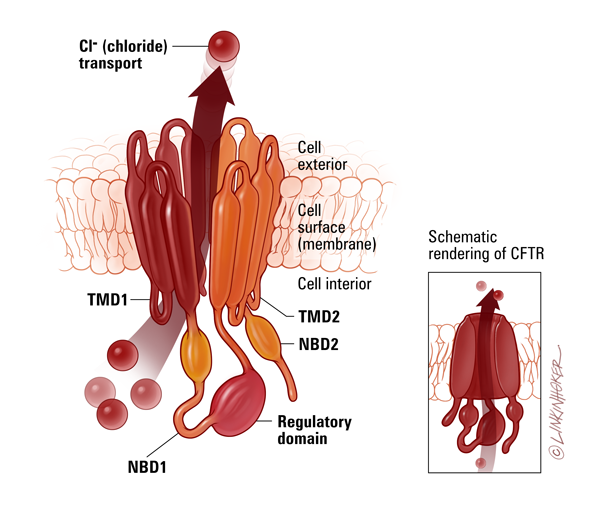
Transmembrane domains — hydrophobic component of a protein (repels water)
Cytoplasmic nucleotide-binding domains — interactions with nucleotides
Regulatory domain — contains phosphorylation
The CFTR Protein is one of the only chloride channels in the ATP-binding cassette superfamily (ABC Family) — also known as the exporters and importers. Not only does it transport chloride, but also other molecules, such as bicarbonates. This protein is made from a gene, called the CFTR gene, which’s located in chromosome 7, position 31.2, and since the discovery of the disease, over 2000 mutations have been found. The defaults of a CFTR Protein (chloride channel) can have major effects on its neighboring channels.
Yes, there’s more than one channel, and each channel has a specific set of jobs and channels for certain molecules.
The abnormal changes in the CFTR protein can affect different channels mainly:
- Chloride bicarbonate exchanger: transports bicarbonates
- CFTR channel: channels chloride
- ORCC: outwardly rectifying chloride channel
- ENaC: epithelial sodium channels
- CaCC: Calcium-Dependent Chloride Channel
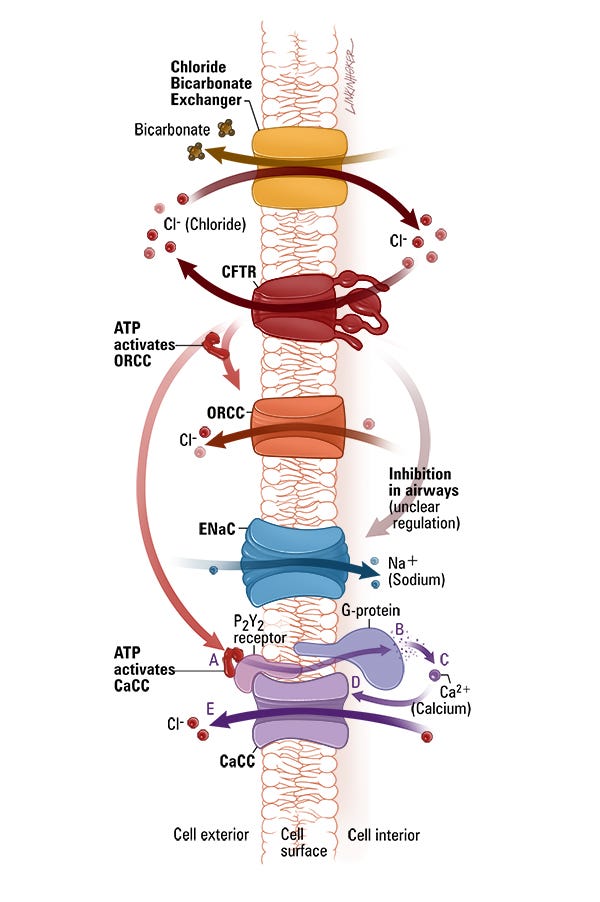
The ORCC consumes ATP molecules to gain energy, through the help of a normal CFTR protein.
ENaC is located on the surface of epithelial cells and is composed of 4 main parts: 2 alpha, 1 beta, and 1 gamma.
the chloride/bicarbonate exchanger transports one bicarbonate molecule out of the cell for every chloride that it transports into the cell. The chloride is derived from the chloride through CFTR.
The CaCC channel is modulated by the P2Y2 receptors, which are activated by ATP molecules.
Pathophysiology of Cystic Fibrosis
Have you ever had a copycat as a friend? If you haven’t, it feels like there are literally 2 of you, since a person (your clone) is repeating almost every single movement of yours. In cystic fibrosis, it’s the same concept but with substances, sodium, chloride, and water.
Sweat Gland
Before sweat enters the skin surface, it is excluded and reabsorbed multiple times. Some quantity of the solution that is brought into space is brought back into a cell, and the remaining of the solution, known as a hypertonic solution, is brought into the surface of the skin, and converted into a liquid substance, called sweat. This process is important, since it balances the components to sweat, by extracting excess amounts of the element.
Meanwhile, a person with CF experiences rejections during secretions. Sodium, chloride, and water are excluded but aren’t reabsorbed. Since chloride channels (CFTR Proteins) are dysfunctional, it doesn’t transport chlorides, as a result, there is an elevated quantity of chloride. This mixture is a hypertonic solution, and since it wasn’t successfully reabsorbed, it leaves as a hypertonic solution. For this reason, a CF patient tends to have saltier skin and sweat. (One of the cystic fibrosis diagnosis includes the sweat test. A patient’s sweat is stored, and the percentage of element mixed is recorded and studied.)
Lung Secretions
Remember when we talked about mucus? Yeah, the icky substance is painted on some parts of our organs. Though it may not be the most appealing thing, it still does help a lot, specifically in cleaning. The mucus in our lungs, need to have certain qualities to work efficiently.
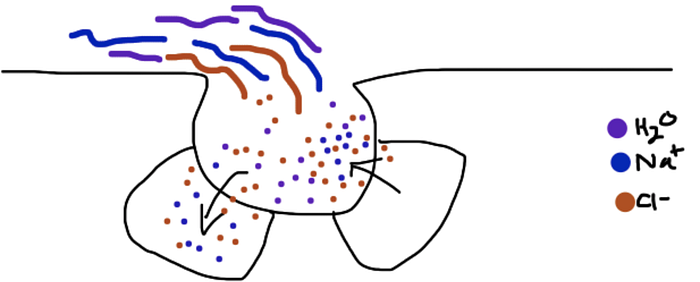
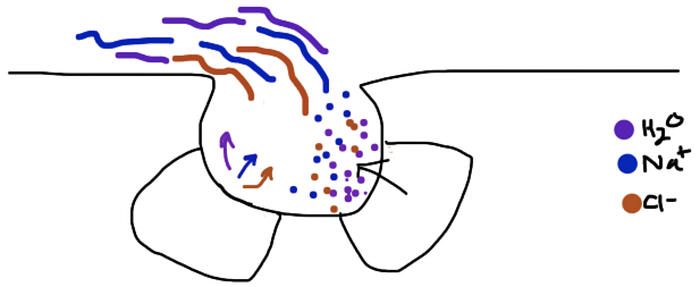
In healthy secretions, chloride is secreted, while sodium and water are reabsorbed. When chloride is brought out of a cell, it attracts water. This water is used to give the mucus a less viscous texture. Cystic Fibrosis secretions is a much more complicated process.
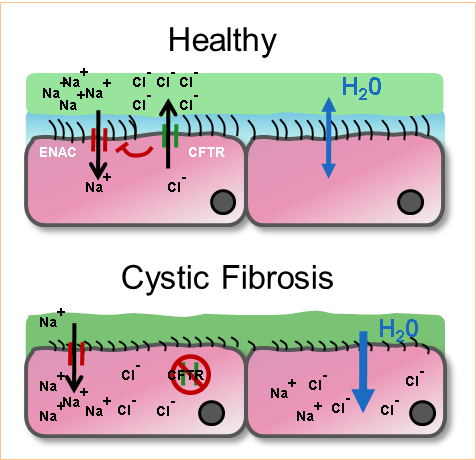
Since the CFTR Protein (chloride channel) is damaged, chloride ions are trapped inside a cell. Being loyal friend sodium is, most sodium stays inside the cell, and so does water. Thereby, there is an increase in sodium and water in the cell. Without chloride attracting water, the mucus becomes dehydrated. With an almost rock-hard material, the cilia don’t have enough strength to push the mucus out of the airway.
The buildup of mucus is a huge barrier to have a healthy body since it acts like a big truck causing some terrible traffic. Researchers and scientists have begun implanting personalized methods to solving this disease. Having a more accurate approach can lead to healthier solutions, and one of the best ways to cure a disease is to have a treatment that is individualized for patients.
Aspects of Cystic Fibrosis
- Genomics: the study of genes — CFTR Gene mutation
- Metabolomics: the study of molecules
- Proteomics: the study of proteins
- Microbiome: genetic material of all the microbes — bacteria, fungi, protozoa, and viruses
- Pharmacogenomics: the study of how genes affect responses to a drug
The main problem for cystic fibrosis is that there isn’t a chloride channel that works properly. Drugs and medications are being developed at the moment, and these are known as modulators. The goal is to create a chloride channel that successfully transports chloride in and out of a cell.
3 types of modulators:
- Potentiators
Chloride isn’t able to travel, since the CFTR channel is closed (like a gate). The purpose of this modulator is to open that gate on the cell membrane, to allow the flow of chlorides. An example of a potentiator is a drug called, ivacaftor.
2. Correctors
The modulator, correctors, are used to fix the shape of the 3D shape of the protein. The CFTR protein needs to hold a specific shape to function, or it dies. Correctors help form the right shape for the protein. As a result, the protein locates itself to the cell membrane.
3. Amplifiers
Amplifiers increase the amount of CFTR proteins made in a cell. The genetic code that instructs the protein structure is multiple, and multiple proteins are created. If there are damaged CFTR Proteins, it can be substituted, by other proteins.
Researchers are trying “therayping” where they develop treatments and drugs, to solve mutations that lead to cystic fibrosis. The primary goal of theratyping is to identify which mutations respond to certain CFTR modulators. This way, helping people with rare CFTR mutations can gain access to approved CFTR modulators quickly and safely.
Cystic Fibrosis isn’t as common, as another disease, such as cancer, or ischaemic heart disease, but the effects can be dangerous. Children who have CF, are restricted in many ways. From foods to exercises, and much more. The lifespan of a cystic fibrosis patient, is within their 30s, leaving them with an extremely short life. In fact, cystic fibrosis is a huge factor in shortened life expectancy. Patients are unable to do “normal” things, this includes breathing!! Cystic fibrosis has been here for almost a century, but it’s about time it goes away
